Sealing the root canal system with a durable and bacteria-tight material guarantees a successful endodontic treatment in the long run. Easier said than done, if you consider the complex nature of the given dental anatomy. The following case report demonstrates that a reliable obturation of the root canal system sometimes just needs a little unusual pressure, i.e. negative pressure.
After having shaped and cleaned the canal, the endo specialist seeks to obturate the prepared space effectively. For this purpose, a number of innovative fast flowing filling materials are already available on the market. However, multiple canals, hidden accessory canals or lateral branches make it difficult to create a permanent seal against bacteria and fluids that can just re-enter the root canal system. Irregularities like culs-de-sac or isthmi are not easy to spot, let alone to be filled properly. A new, simple technique using standard instruments can help practitioners to get the job done in no time. All you need is free-flow filling material and a new, special endodontic aspirating tip to create a bit of negative pressure, as my latest endodontic case shows.
Case Report
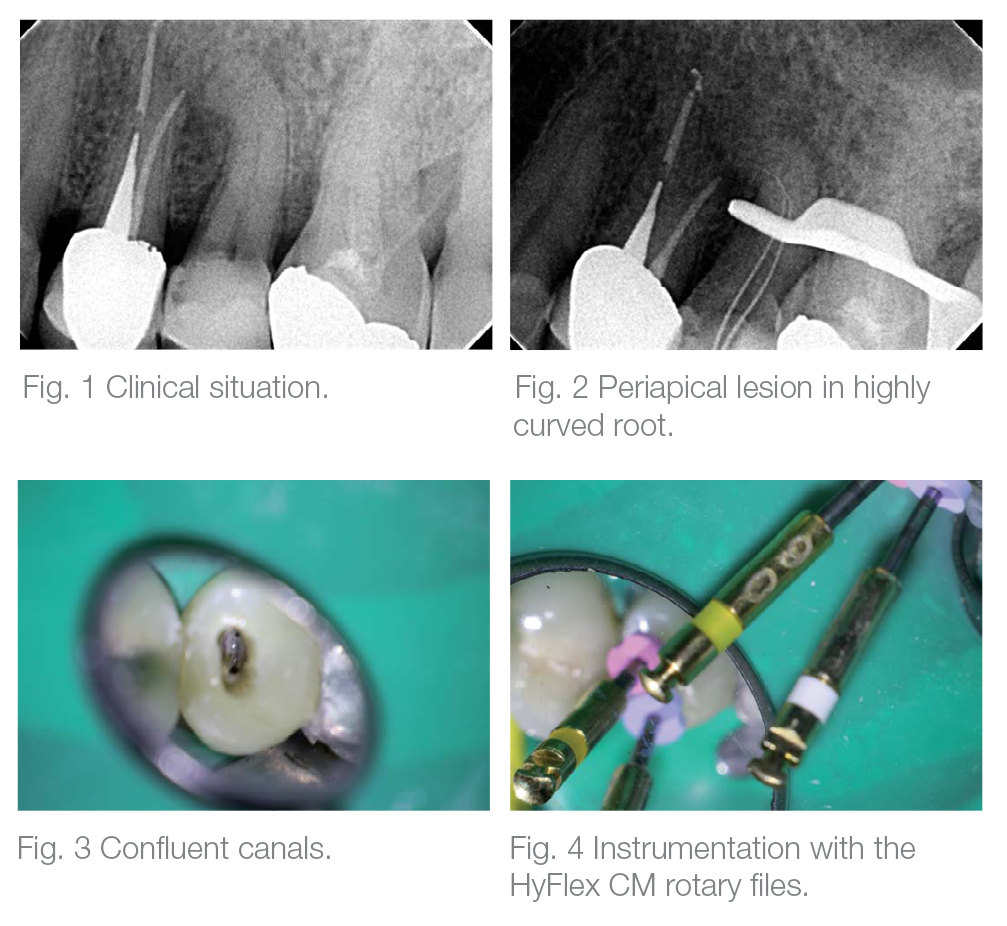
A 50-year-old male patient was referred to my endodontic practice for evaluation and possible treatment of his left maxillary second premolar. The tooth was percussion painful and a buccal swelling was evident. Endo-Ice cold vitality testing was negative. Radiographic examination, moreover, revealed a periapical lesion associated with a highly curved root (Figs. 1 & 2). The pulp was consequently diagnosed as necrotic and the periapical diagnosis was consistent with Symptomatic Apical Periodontitis (SAP).
After placing the rubber dam, the pulp chamber was accessed with a diamond DiaDent bur under microscopic visualisation. Two confluent canals were identified and length determination radiograph revealed the highly curved canal anatomy (Fig. 3). Length was verified using the CanalPro Apex Locator. Instrumentation was then achieved with the Hyflex CM rotary files used in a single length protocol. After flaring with 25/0.8, the rotary file sequence followed consisted of 15/0.4, 20/0.4, 25/0.4, 20/0.6 and 30/0.4 to length. After the instrumentation procedure a radiograph confirmed that the original trajectory was maintained (Fig. 4). The angulation of the aforementioned periapical radiograph revealed two lateral lesions suggesting two lateral portals of exit (Fig. 5). The canals were rinsed after each change of instruments according to a strict irrigation protocol. Two corresponding 30/0.4 gutta-percha master cones were then fitted to the canals. The rinsing solution was activated by using dynamic manual agitation with the master gutta-percha cones (holding the cone with tweezers to gently move it up and down).
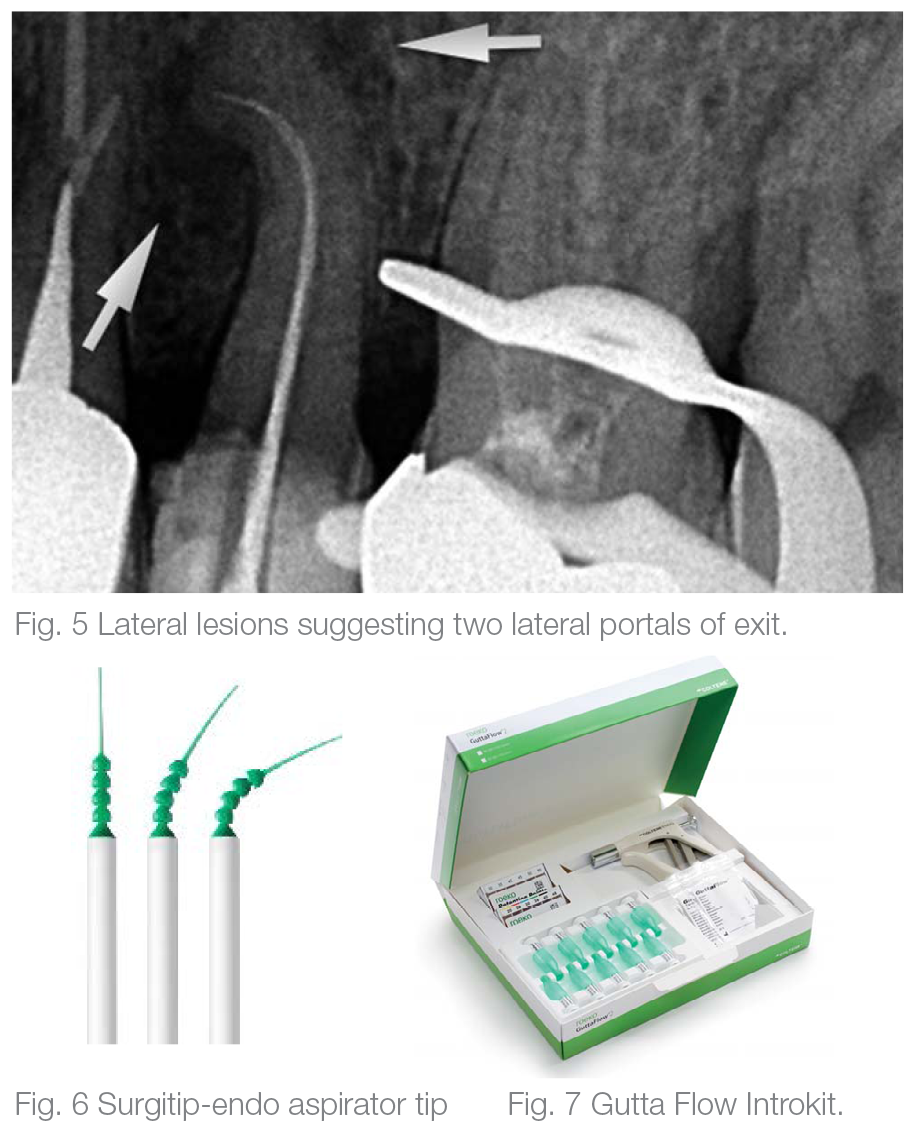
During this process, an endodontic aspirator tip was used to dry the root canals. The Swiss dental specialist Coltène/Whaledent introduced an aspirating tip specially developed for drying root canals. With an outer diameter corresponding to ISO 60, the Surgitip- endo can be inserted directly into the prepared canal where it removes rinsing solutions and other moisture quickly and effectively at the same time. Thanks to a special fully rotating ball joint, the suction tip is highly flexible and collapsing of the tip is therefore avoided (Fig. 6). You can easily fit it into root canals that are normally hard to reach without having to bend the canal tip. After drying the confluent canals, the Surgitip-endo was fitted to the buccal canal orifice and the irrigation solution was injected in the lingual canal. Simultaneous negative and positive pressure irrigation from different orifices created a continuous current of fresh irrigant washing out all debris.
In the next step the preparation for negative pressure filling of the root canal system was taking place.
This special filling system was created with the use of the Surgitip-endo and the tight seal material GuttaFlow 2 (Fig. 7). This filling material combines cold free-flow gutta-percha and a sealer creating an easy to handle, fast flowing filling material, which has been proven as a reliable barrier against bacteria and liquids re-entering the root canal. Its working time takes approximately ten to fifteen minutes. Before the actual procedure starts, it is necessary to fix both the Surgitip-endo front part as well as the CanalTip of the GuttaFlow capsules at the entrance of both canals. Both the front part of Surgitipendo and a canal tip are firmly fixed in the different orifices by a sealing material that is polymerised for approximately 10 seconds (Fig. 8). The seal at the canal entrance works as a temporary cap to enable the establishment of negative pressure underneath it with the aid of the aspirating tip. With this special trick a negative pressure zone can be created, which allows literally to pull the gutta-percha filling material into smaller lateral canals and ramifications that were hardly detectable in the anamnesis before.
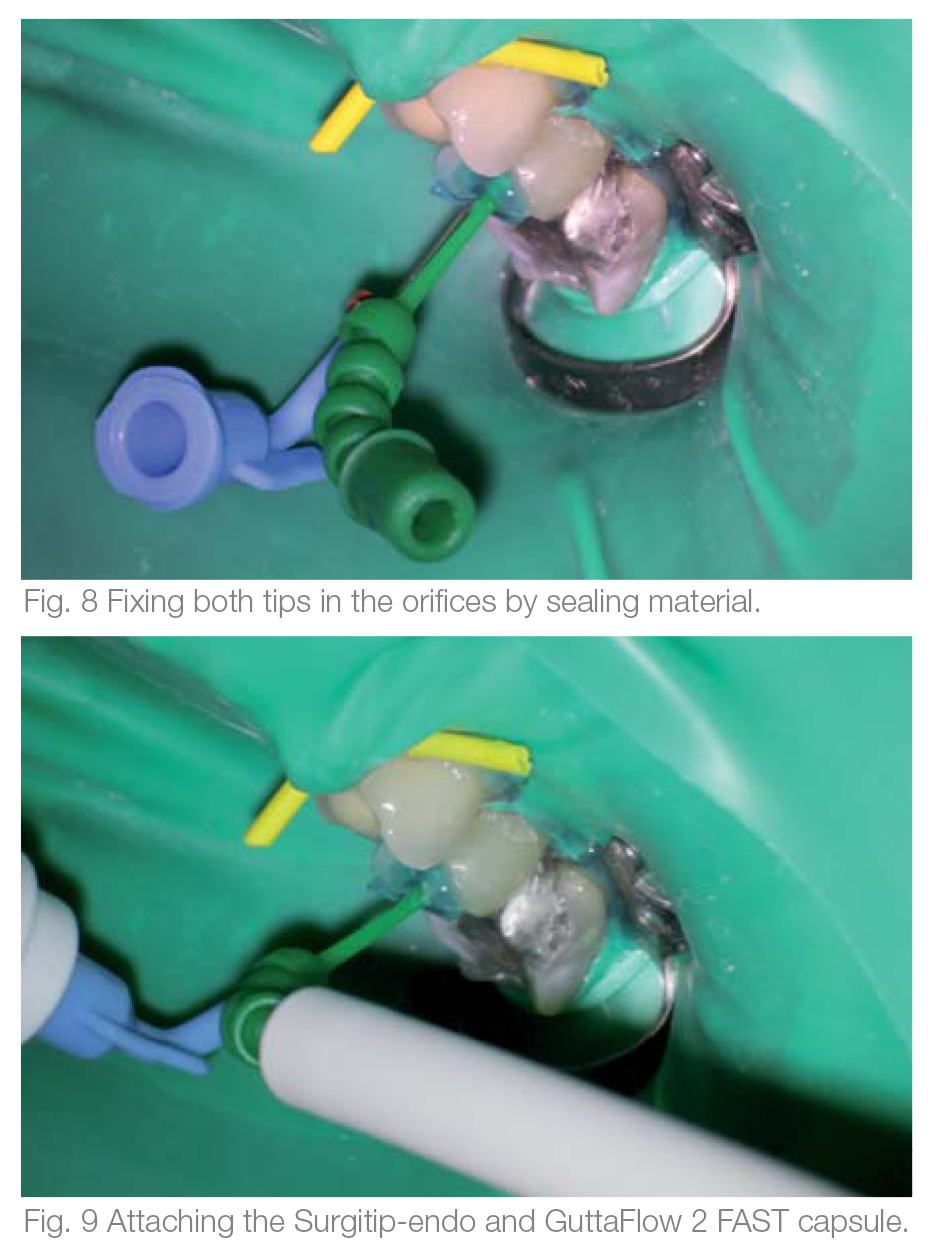
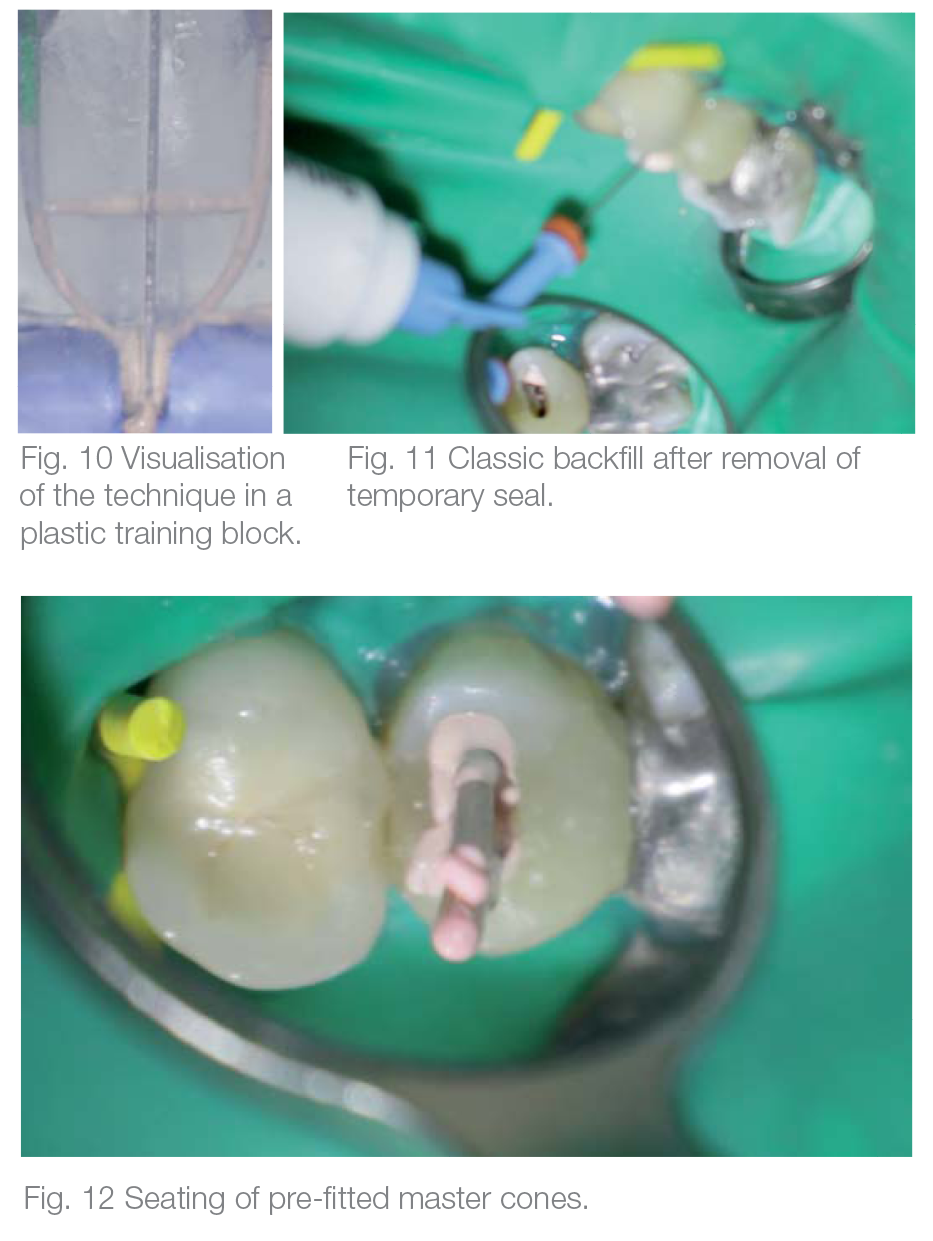

Now a GuttaFlow 2 FAST capsule was attached to the CanalTip as well as the Surgitip-endo to its front part (Fig. 9). While the air was sucked off with the Surgitip-endo above the filling, the guttapercha material was released into the canal system simultaneously and quickly spread into the prepared root canal system. In general, the innovative design of the suction tip ensures unrestricted high suction performance at all angles, therefore the gutta-percha was evenly distributed and filled the confluent canals within seconds. Complete control of the material extrusion was consequently achieved (Fig. 10). After the injected GuttaFlow 2 had reached the Surgitipendo, the temporary sealing material could be removed. The rest of the GuttaFlow 2 capsule was used for a classic backfill and the pre-fitted master cones were very slowly seated in place (Figs. 11–13).
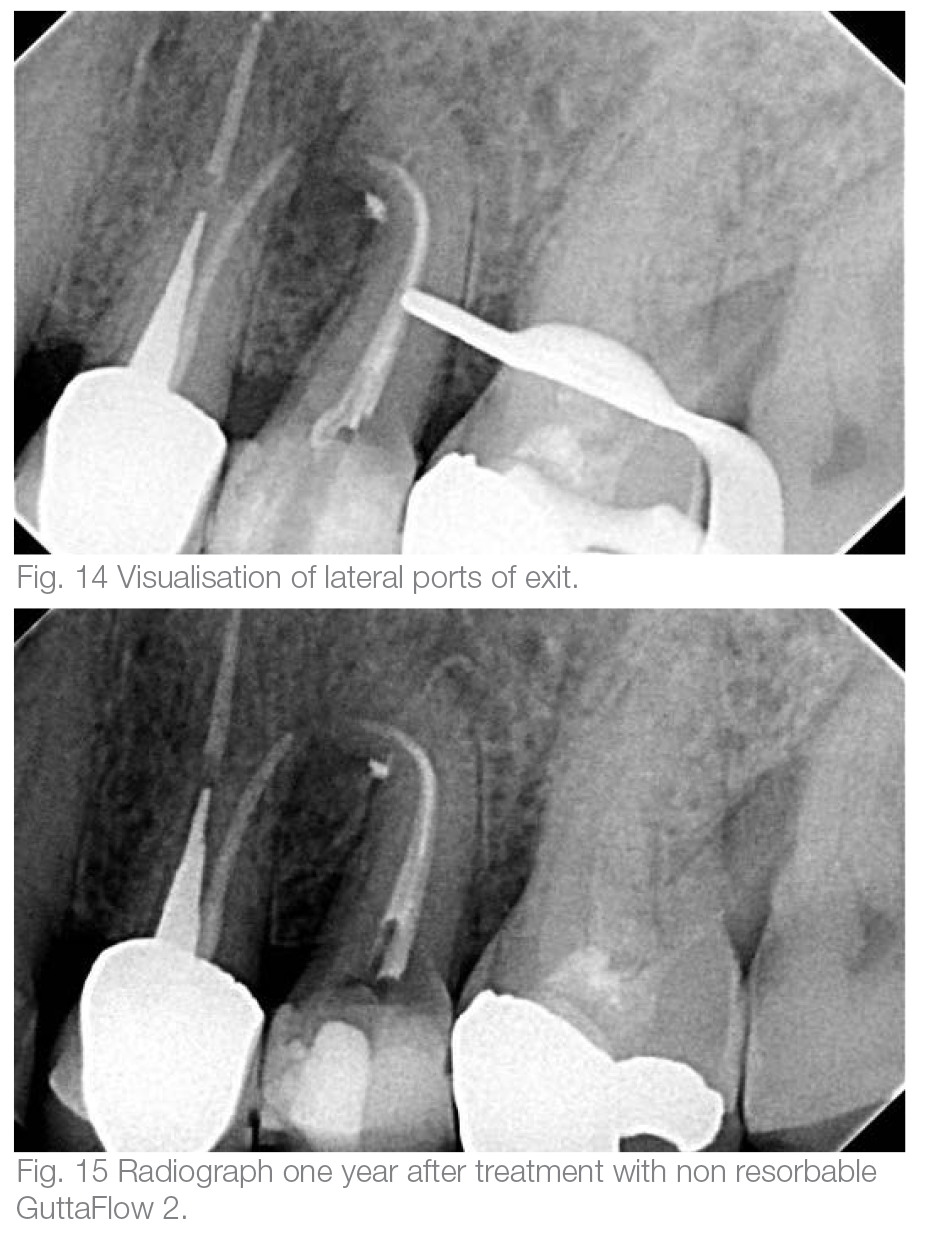
The tooth was restored with a fiber post, a composite built up and a PFM crown. In the final radiographic image of the tooth right after the RCT, the lateral ports of exit could be visualised (Fig. 14). One year after the treatment, the follow-up radiograph revealed complete healing. The nonabsorbable GuttaFlow 2 could be detected unaltered in the lateral portals of exit (Fig. 15). The buccal and occlusal clinical view of the tooth and soft tissues can be seen in Figures 16 and 17.

Conclusion
Innovative filling systems nowadays come with excellent flow properties. They are easy to handle and help to speed up treatment sessions, even more so if dentists make good use of their endodontic instruments. Creating a negative pressure zone with a special endodontic aspiratory tip is easy to learn, but saves additional time in the process. No extra material or instruments are needed. The guttapercha is easily distributed to the root canal system, even in areas that are hardly detectable beforehand and often impossible to fill. The combination of modern equipment and individual craftsmanship thus guarantees a tight seal of the root canal for an optimum protection against re-infection. Negative pressure obturation with GuttaFlow 2 provides absolute material control and a fluid tight seal of the main root canal system and its lateral components.
Article Published Feb - Mar 2024 Dental Solutions
Reference
(2014) ROOTS ‘Industry Report _ Innovative Filling Systems’, Volume 3, Pgs 14-17.